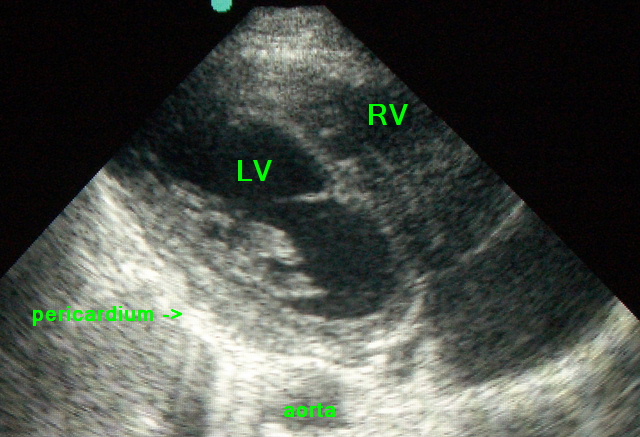
Echo of normal heart – Parasternal View – labeled
****
ED Echo: Basics
- Positioning: Elevate the head of bed slightly, have the patient bend their knees to get a better and less uncomfortable subcostal/subxiphoid view.
- Sub-Xyphoid View: Remember to angle the ultrasound beam under the patients xiphoid process and towards their left shoulder.
- Parasternal Views: Place the probe to the left of the sternum. Having the patient twist their torso to the left can help bring the heart closer to the chest wall and away from their sternum, therefore improving your parasternal views.
Want more educational images? Check out the ED Atlas on CD
****
Echo of normal heart – Parasternal View – labeled
****
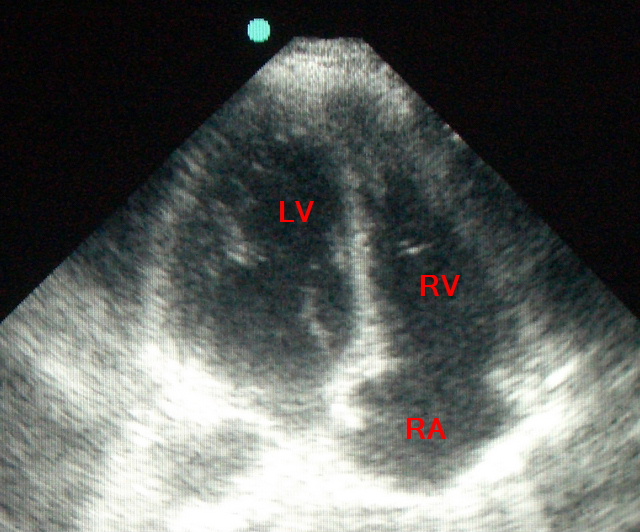
Echo of normal heart – Apical View – labeled
****

Normal Heart: Sub-xyphoid veiw
****
Dilated Heart from advanced CHF
****

Amyloid Heart: note thick walls
****
ED Echo: Pulmonary Embolism
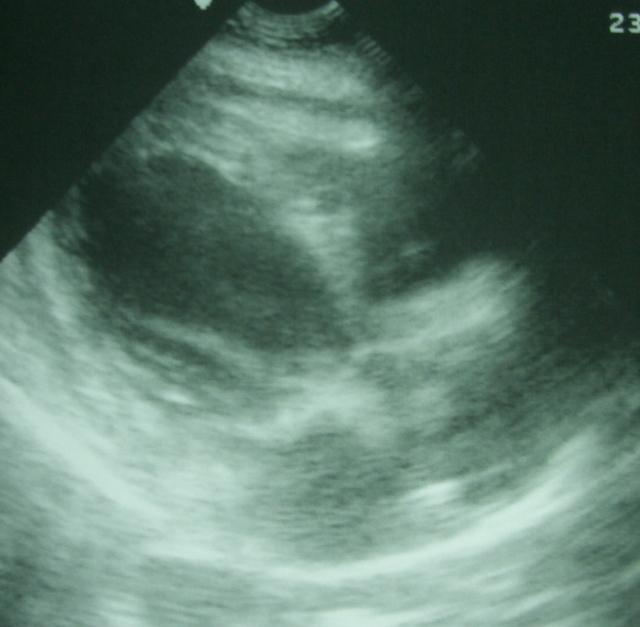
- Pulmonary Embolism: Look for dilated right ventricle (RV), which will be anterior. The RV often cannot contract well due to the distal obstruction. Rarely you may actually see clot in the RV.

Pulmonary Embolism causing dilated hypokinetic Right Ventricle
****

Pulmonary Embolism causing dilated hypokinetic Right Ventricle
****
Pulmonary Embolism causing dilated hypokinetic Right Ventricle
****
ED Echo: Pericardial Effusions
- Pericardial Effusions: Make sure you visualize the posterior pericardium surrounding the heart. Gravity will direct small amounts of pericardial fluid to accumulate in the posterior pericardium in patients who are lying supine. Remember that fluid doesnt accumulate behind the left atrium because the pericardium is adherent to the myocardium there. A hypoechoic space seen anterior to the heart with no evidence of posterior fluid is most likely a pericardial fat-pad, however, a loculated effusion is possible. Learn how to perform both parasternal and subxiphoid scans so comparison views can be obtained in cases that are not cut and dry. Beware, pleural fluid can be mistaken for pericardial fluid. If uncertain, try to visualize the aorta behind the heart. If the fluid is posterior to the aorta it is likely pleural, rather than pericardial, in origin.
- Pericardial Tamponade: Echocardiographic findings in pericardial tamponade include diastolic right atrial and/ or right ventricular collapse. These finding are usually seen prior to the clinical picture of tamponade (hypotension, tachycardia, jugular venous distension)
- Pericardiocentesis: Use bedside ultrasound to help you determine where the largest collection of fluid has accumulated. The apex is usually the best site to start, but look everywhere to be certain. The traditional subcostal approach is best in only 12% of cases. Scan around the thorax until you find the location where you maximize your chances of tapping into the effusion, meanwhile minimizing the chance of accidentally puncturing an organ.

Cardiac Tamponade: Malingnant
****

Pericardial Effusion
****
ED Echo: IVC & Volume Status
****
Do you want a pocket reference that has essential material on ED Ultrasound as well as other imaging, labs, EKG’s, procedures, risk management and more?
Then get the 8-in-1 Emergency Department Quick Reference
****
WOULD YOU LIKE TO USE ONE OF OUR IMAGES?
As long as you paste the following statement with a weblink to this site, no problem: “Image reproduced with permission, ERPocketBooks.com”
****
WOULD YOU LIKE TO USE ONE OF OUR IMAGES?
As long as you paste the following statement with a weblink to this site, no problem: “Image reproduced with permission, ERPocketBooks.com”
****