History of Present Illness: A man in his late 60’s with a history of valvular heart disease, BPH and bipolar disorder presents to the ED for 5 days of gradually worsening dizziness, shakiness and generalized weakness with multiple falls. He denies any injury from the falls. He denies any fever, nausea, chest pain, SOB or other complaints.
Vital Signs & Physical Exam: Vital signs are normal. Physical exam is otherwise normal except for the oropharynx, which seems somewhat dry. He also has some teeth grinding and just seems a bit odd
Initial Diagnostic Testing:
- CBC: white count of 12, stable hemoglobin of 11.8 with macrocytic indices
- Chem 7: BUN and creatinine are 46 and 2.8, which are new. Troponin slightly elevated at 12.
- Imaging: Brain CT normal
- EKG: see below
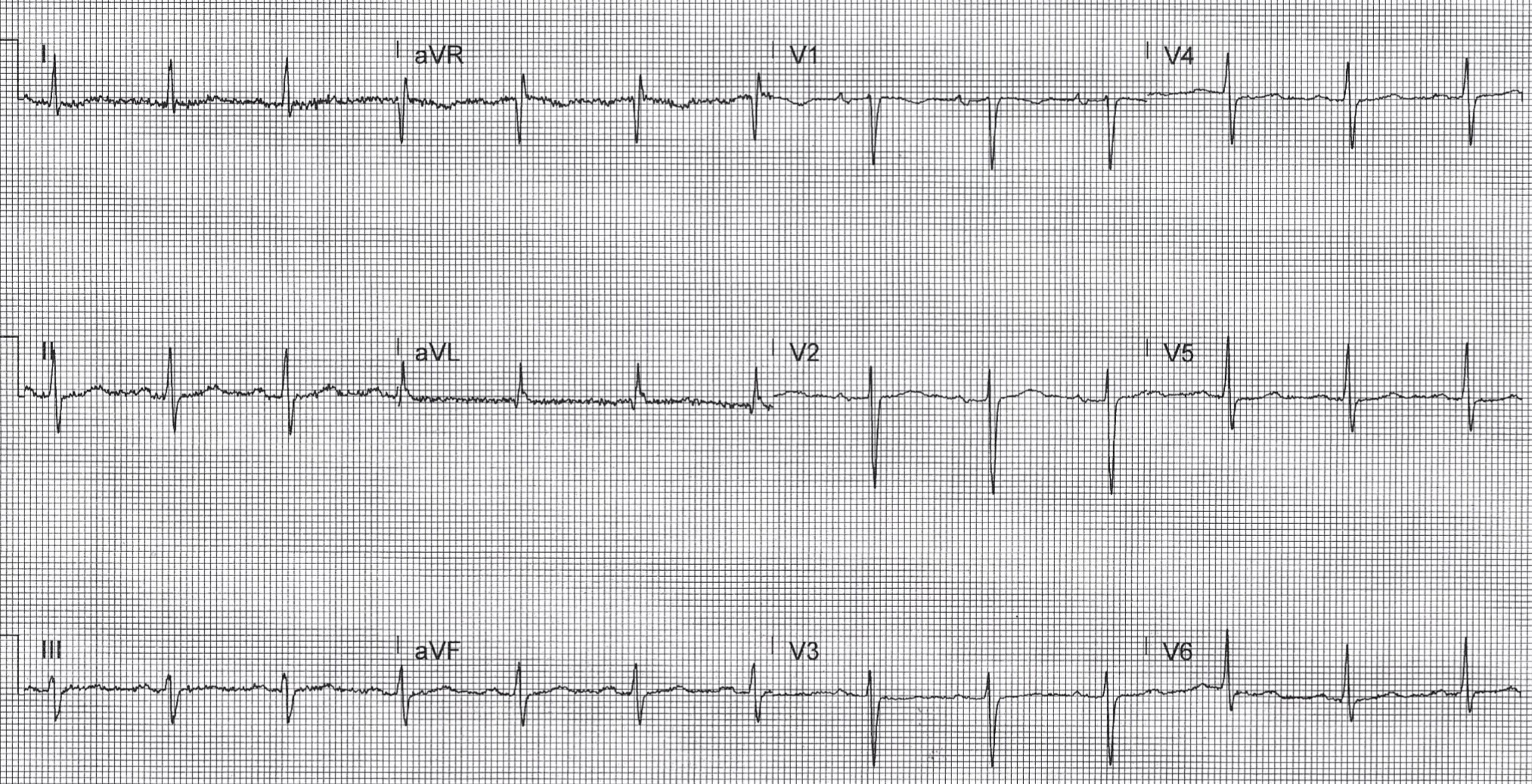
Computer Read: NSR at 76, first degree AV block, IVCD, non-specific T wave abnormality
What is the most likely cause of ECG findings in this patient?
- A) Acute coronary occlusion
- B) Blood clot (PE)
- C) Cardiac tamponade
- D) Drug toxicity
- E) Electrolyte issue
SCROLL DOWN FOR THE EKG ANALYSIS & 1-MINUTE CONSULT
<<<<<<<<<<<<<<<<<<<<< ADVERTISEMENT & SPACER >>>>>>>>>>>>>>>>>>>>>
THE EMERGENCY MEDICINE POCKETBOOK TRIFECTA

- Emergency Medicine 1-Minute Consult, 5th edition
- A-to-Z EM Pharmacopoeia & Antibiotic Guide, NEW 5th edition
- 8-in-1 Emergency Department Quick Reference, 5th edition
******************************************************************************
<<<<<<<<<<<<<<<<<<<<<<<<< END SPACER >>>>>>>>>>>>>>>>>>>>>>>>>
My ECG interpretation: Computer interpretation is correct (first degree AV block, IVCD, non-specific T wave abnormality) but there is also some fine tremor artifact. Also, it is a bit unusual that the heart rate is only 76 given the BUN and creatinine level.
ANSWERS:
- A) Acute coronary occlusion – good thought
- B) Blood clot (PE)
- C) Cardiac tamponade
- D) Drug toxicity – CORRECT – he forgot to tell anyone he was on lithium
- E) Electrolyte issue
1-Minute Consult on the topic for this case from the Emergency Medicine 1-minute Consult Pocketbook
CASE CONCLUSION: Lithium level was critical at 1.8 (normal 0.6-1.2)ECG changes in Lithium can include the following: Tremor artifact, T-wave flattening >T-inversion >AV block, IVCD, ST elevation, long QT. He was admitted and treated with IV fluids. His symptoms gradually improved
CASE LESSONS:
- Always consider medication toxicity in drugs where levels are monitored.
- Consider medication side effect after ruling out other causes.
- Ask patient’s with bipolar if they are taking Lithium even when it is not listed on their medication list.