History of Present Illness: A woman in her mid-20’s presents to the urgent care with approximately 5 days of pleuritic right upper quadrant pain. She denies any fever cough or shortness of breath. She has also been having epigastric pain that is non-pleuritic and is not as severe as the right upper quadrant pain. She has never had this before. Approximately 3 weeks ago she took Plan B for unprotected sex and motrin for a bad period. She denies any vaginal discharge or lower abdominal pain. No dysuria, melena or other complaints.
Vital Signs & Physical Exam: Vital signs are normal. Physical exam is otherwise normal except for epigastric tenderness
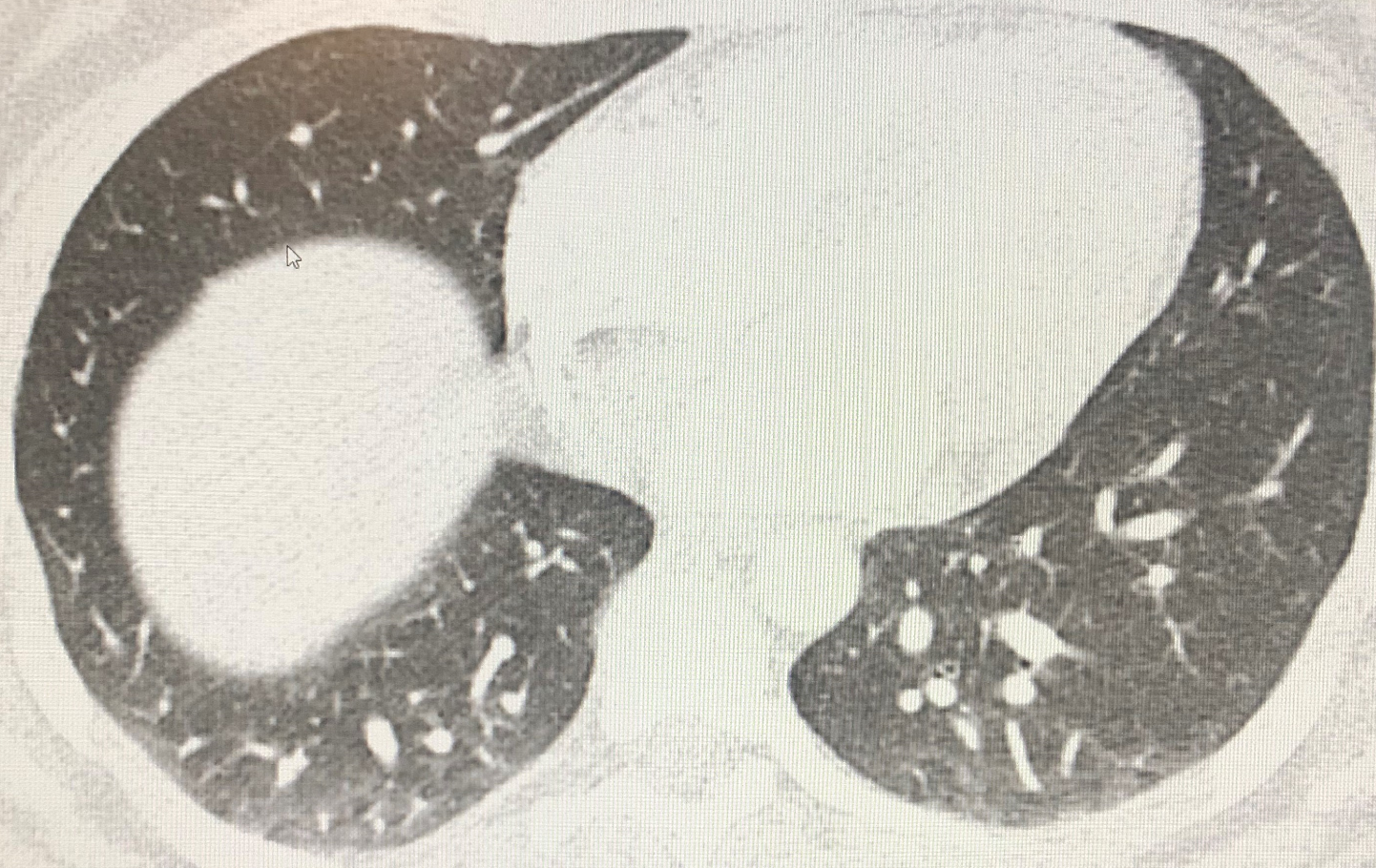
Initial Diagnostic Testing: Pregnancy test negative. CBC normal except for white count of 14.1. Metabolic panel essentially normal as was urine except for 5 red cells. ALT elevated at 167 with an AST of 48. Ultrasound shows no gallstones, only a fatty liver. Chest x-ray normal. D-dimer quite elevated >2,500 prompting a CT scan, which showed no pulmonary embolism (see image below)
What is the most likely cause of the RUQ pain?
- A) Coxsackie B virus
- B) Hepatitis B virus
- C) Fatty liver disease
- D) H. pylori
- E) C. trachomatis
SCROLL DOWN FOR ANSWERS & 1-MINUTE CONSULT
<<<<<<<<<<<<<<<<<<<<< ADVERTISEMENT & SPACER >>>>>>>>>>>>>>>>>>>>>
THE EMERGENCY MEDICINE POCKETBOOK TRIFECTA

Emergency Medicine 1-Minute Consult, 5th edition
A-to-Z EM Pharmacopoeia & Antibiotic Guide, NEW 5th edition
8-in-1 Emergency Department Quick Reference, 5th edition
******************************************************************************
<<<<<<<<<<<<<<<<<<<<<<<<< END SPACER >>>>>>>>>>>>>>>>>>>>>>>>>
ANSWER: What is the most likely cause of the RUQ pain?
- A) Coxsackie B virus – POSSIBLE – Bornholm disease, also known as epidemic pleurodynia, is a condition characterized by myositis of the abdomen or chest caused by the Coxsackie B virus or other viruses.
- B) Hepatitis B virus – UNLIKELY – can cause elevated LFT but is typically painless
- C) Fatty liver disease – UNLIKELY – can cause elevated LFT but is typically painless
- D) H. pylori – UNLIKELY – does explain the epigastric pain and tenderness after ibuprofen use
- E) C. trachomatis – CORRECT – the most common presentation for Fitz-Hugh-Curtis perihepatitis is pleuritic RUQ pain with elevated D-dimer and negative CT. LFT’s are usually normal therefore the LFT results here are likely unrelated and instead from the fatty liver. Although classically FHCD includes pelvic symptoms of the roughly 1 case per year that I have diagnosed over the past 20 years, only one had any pelvic symptoms and that was the one that was from gonorrhea rather than chlamydia trachomatis.
1-Minute Consult: Click HERE and scroll to the BOTTOM of page 90.
CASE CONCLUSION: CT scan showed only atelectasis. Epigastric component of pain relieved by Maalox. Treated empirically for STD. Chlamydia came back positive the next day.
CASE LESSONS: learn this presentation so as not to miss this diagnosis (like most providers probably do most of the time). In summary the presentation includes:
- female, usually young, with recent unprotected sex, and pleuritic RUQ pain,
- elevated D-dimer with normal CTPA.
- WBC and LFT’s usually normal but CRP/ESR often elevated.