History of Present Illness: A man in his early 70’s with DM and HTN presents with 2.5 hours of heartburn associated with nausea and chills. He has been having similar symptoms on and off for the past few days which have been relieved by Mylanta, but today it got worse despite Mylanta. He denies SOB, vomiting, diarrhea or abdominal pain but does feel a bit light headed
Vital Signs & Physical Exam:
Vital signs are normal except for a slightly elevated BP. Abdomen is non-tender. The rest of the exam is normal although he seems a tad sweaty
An ECG is done
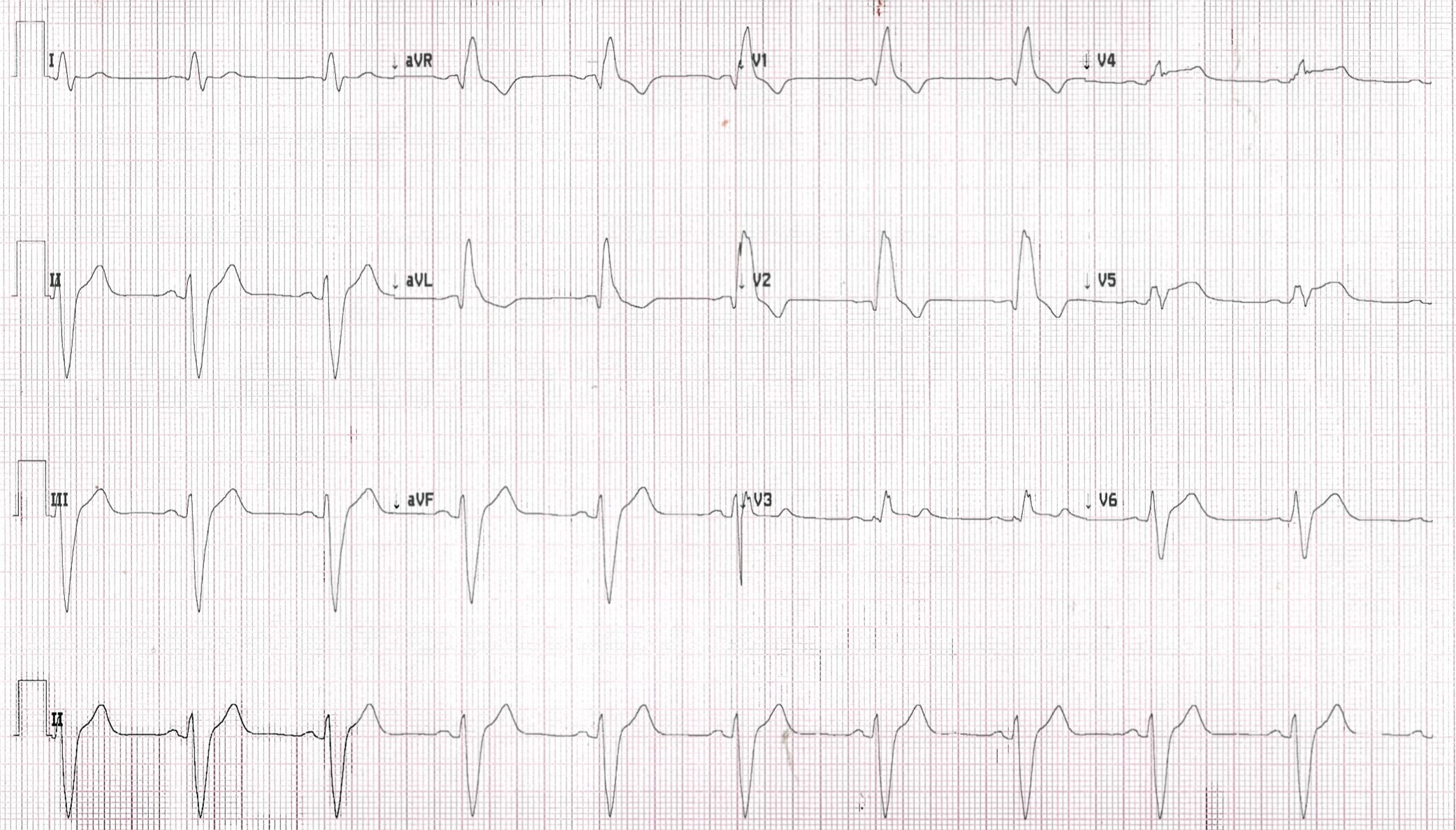
Computer Read: NSR, IVCD, NSSTC
What is the most likely cause of the ECG findings in this patient?
- A) Gastritis
- B) GERD
- C) Cardiac: ACS
- D) Gallstones
- E) Electrolyte abnormality
SCROLL DOWN FOR ANSWERS & 1-MINUTE CONSULT
<<<<<<<<<<<<<<<<<<<<< ADVERTISEMENT & SPACER >>>>>>>>>>>>>>>>>>>>>
****************************************************************************
THE EMERGENCY MEDICINE POCKETBOOK TRIFECTA

Emergency Medicine 1-Minute Consult, 5th edition
A-to-Z EM Pharmacopoeia & Antibiotic Guide, NEW 5th edition
8-in-1 Emergency Department Quick Reference, NEW 5th edition
******************************************************************************
<<<<<<<<<<<<<<<<<<<<<<<<< END SPACER >>>>>>>>>>>>>>>>>>>>>>>>>
QUIZ ANSWER: What is the most likely cause of the ECG findings in this patient?
- A) Gastritis
- B) GERD
- C) Cardiac: ACS – CORRECT, had a 99% ostial LAD occlusion on cath
- D) Gallstones
- E) Electrolyte abnormality
My ECG interpretation: Pretty wide QRS. ST elevation V3-V6
1-Minute Consult on this topic: Click HERE and scroll to proper page
Case Outcome:
-
- Code STEMI called. Cath showed proximal LAD occlusion
- First troponin was already 715 and peak was >5000
- Echo showed EF of 35%
- Heart block developed so he had an AICD/Pacer placed
Lessons:
- Heartburn relieved by antacids may actually be unstable angina that goes away on its own and has nothing to do with the antacid
- Diaphoresis is always a red flag