History of Present Illness: A man in his mid-60’s with ESRD and mild dementia presents to the hospital with severe generalized abdominal pain that started right after finishing dialysis and was associated with vomiting but no fever, diarrhea or other complaints. He is a poor historian.
Vital Signs & Physical Exam: Vital signs are normal except for somewhat elevated blood pressure. Physical exam is notable for a patient who is agitated and yelling in pain and threatening to walkout. He later pulled out his IV and tried to leave
Initial Diagnostic Testing:
- CBC: normal except for WBC 9.5 (baseline for him ~5.0) and Hb 10.5 (his baseline)
- Chem-7: normal except for bicarb 22 (baseline 28 after dialysis) but anion gap of 21
- Imaging: see plain film below
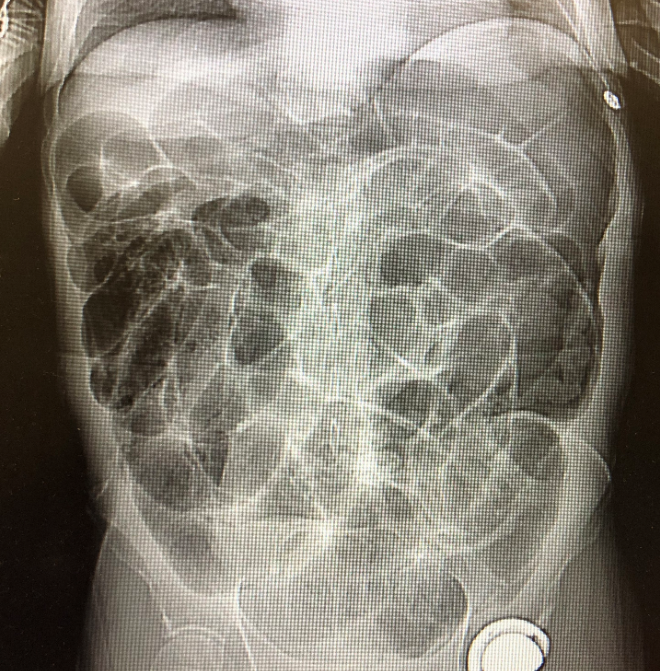
Why is it wise to do a plain film in a patient with excruciating abdominal pain?
- A) look for free air
- B) look for volvulus or mesenteric ischemia
- C) look for SBO
- D) minimize radiation exposure
SCROLL DOWN FOR ANSWERS & 1-MINUTE CONSULT
<<<<<<<<<<<<<<<<<<<<< ADVERTISEMENT & SPACER >>>>>>>>>>>>>>>>>>>>>
THE EMERGENCY MEDICINE POCKETBOOK TRIFECTA

- Emergency Medicine 1-Minute Consult, 5th edition
- A-to-Z EM Pharmacopoeia & Antibiotic Guide, 5th edition
- 8-in-1 Emergency Department Quick Reference, 5th edition
***************************************************************************
Check out our Weekly EM Case Challenge
We’re currently posting on Facebook (ERpocketbooks.com) & Twitter (@EM1MinuteGuru) twice a month
<<<<<<<<<<<<<<<<<<<<<<<<< END SPACER >>>>>>>>>>>>>>>>>>>>>>>>>
ANSWER: Why is it wise to do a plain film in a patient with excruciating abdominal pain?
- A) look for free air – CORRECT. Note that patients with a perforation usually try to stay extra still and don’t act agitated like this
- B) look for volvulus – ALSO CORRECT. If a patient is screaming with excruciating abdominal pain it is probably drama but consider that they may have ischemic bowel. Sudden bowel ischemia from either a volvulus or mesenteric ischemia can cause people to act very agitated. They may develop an agitated delirium that makes you wonder if they are a psych patient. Plain films are faster and if they show a cecal volvulus you should call the surgeon before CT to minimize the chance of a bad outcome. Mesenteric ischemia will almost always need a CT, but findings on plain film may push you to get the CT faster.
- C) look for SBO – for this you will usually need a CT though plain films may give you an answer sooner and get patients who will need surgery to the OR sooner. Also, if there is low suspicion but you feel you need some imaging for SBO, plain films are quicker and have less radiation than CT. Sensitivity is ~80%, and probably even higher if you call a gasless abdomen positive.
- D) minimize radiation exposure – a consideration in younger patients or with low level of suspicion, but not for this patient.
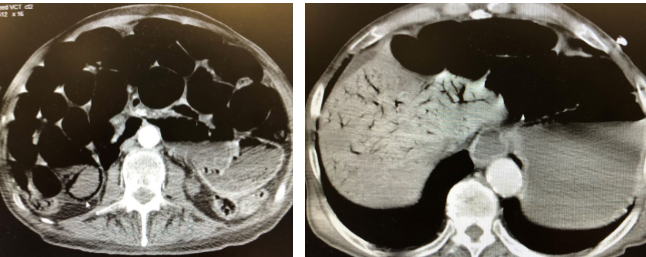
CT cuts below showing pneumatosis in dilated small bowel (white arrowhead near lateral spinous process) and portal venous gas in the liver
1-Minute Consult on this topic: Click HERE and scroll to appropriate page.
CASE CONCLUSION: became progressively more tachycardic and kept vomiting despite fluids and huge doses of pain meds and antiemetics. lactic acid was 6.3. CT showed pneumatosis and portal gas from mesenteric ischemia, as well as a sever ileus. Patient went to the OR and had resection of 65% of the small intestine. Fortunately it had not perforated. Survived and did as well as could be expected.
CASE LESSONS: a borderline WBC or bicarb usually aren’t big red flags, but they can be, especially if they are very different from the patients known baseline value (most patients have a baseline WBC count. It doesn’t just bounce around between 5 and 10.